Traumatic Brain Injury
By Trevor Wilson MD
Head Trauma (Background)
-
Epi: 1.7 million people / year
-
Traumatic Brain Injury (TBI) leading cause of death in North America from 1-45 y/o
-
TBI 15.1 all injury related hospitalizations
-
Causes (civilian): falls (43.7%), MVC (21.5%)
-
Non-civilian: “signature injury” of Iraq and Afghanistan war (10-20%)
-
Sequelae: 5.3 million in US with disability 2/2 TBI
The Landscape
-
Paucity of large RCTs
-
Movement to standardized care
Principles of Disease Process
-
Primary Insult
-
“No effective intervention has been found to reverse the pathologic events initiated by the (primary) traumatic event.” (Rosens’s)
-
public health measures
-
-
Secondary Insult
-
focus of this talk
-
the topic we (EM+Trauma+NS) own
-
where what we do matters
-
Factoids:
-
brain weighs 1.4kg (3lb)
-
consumes 2% of entire oxygen consumed by body, ergo 15% CO
-
pressure of CSF 5 – 15 mm Hg (65-195 mm H20)
-
regulated by vasoconstriction/dilatation which is regulated affected by hypertension, acidosis, hypocarbia (and vice versa)
Pathophysiology (Pertinent)
-
Cerebral Blood Flow (CBF) remains at constant levels w/ MAP 60-150 mm Hg
-
TBI can cause dysfunction of the autoregulatory mechanism. “Pressure-passive”
-
Cerebral Vasoactivity
-
hypotension, by BP, pH, CO
-
CPP = MAP – ICP
-
Goal CPP 60 (50-70) mmHg (Brain Trauma Foundation et al. 2007c)
Focus on management:
Classification of TBI
-
Mild GCS 13-15
-
Moderate 9-12
-
Severe
-
ED Definition:
-
post-resuscitation GCS <=8 on presentation
-
intracranial contusion, hematoma, laceration
-
-
Other non-practical neurosurgical definitions (@ 48 hrs post injury)
-
Cannot prognosticate based upon initial GCS or CT (Marx et al. 2006)
-
Mortality 35% (Marmarou et al. 2007)
-
-
Types
-
Skull fracture, subdural, epidural, subarachnoid, cerebral contusion, diffuse axonal injury
-
Pre-Hospital Care
-
Prevent hypoxia and hypotension
-
IV access
-
Hemostasis with head laceration
-
Risks/benefits for sedation to prevent agitation thereby causing increase in ICP
-
Helicopter if ground >30 min
-
Controversy regarding intubation (Marmarou et al. 2007; Bar-Joseph et al. 2009; Bernard et al. 2010)
-
Successful -> better outcomes
-
Unsuccessful attempts -> hypoxia and prolonged scene time -> worse outcomes
-
RSI if by well-trained EMS. (Marmarou et al. 2007; Bar-Joseph et al. 2009; Bernard et al. 2010; Fakhry et al. 2006)
-
ED Management
-
Airway
-
RSI*
-
Brief neurological exam
-
-
-
Breathing, Circulation, Disability, …ATLS
Optimization of the Medical Resuscitation (Outline)
-
-
Hypotension
-
Hypertension
-
Osmotic agents
-
Barbiturates
-
Steroids
-
Steroids
-
Hypothermia
-
Cranial decompression
-
Seizure Prophylaxis
-
Antibiotic Prophylaxis
-
Priorities
-
-
Low Hanging Fruit for Mitigating Sequelae
-
-
Head of Bed 30 degrees
-
Loosen neck brace, neck in neutral position (venous drainage)
-
Sedation/analgesia
-
Treat anemia (Hb >10mg/dL)
-
Avoid albumin
-
Resuscitate with NS (LR is slightly hypotonic)
-
-
Hypotension
-
Usually hypovolemic
-
Usually no from head but can have profound blood loss from scalp laceration
-
-
Neurogenic if clear high spinal lesion, non-responsive to IVF, inappropriate bradycardia (dx with caution)
-
Tx: SBP >90 mm Hg
-
Aggressive IVF does not increase cerebral edema
-
Traditionally NS or LR
-
Resuscitation Outcomes Consortium: no improvement with hypertonic saline (HTS) (Bulger et al. 2010)
-
-
Hypoxia
-
Goal PaO2 >60 mmHg
-
-
Electrolytes
-
Correct derangements
-
-
Sedation
-
Propofol appears to be associated with trend towards better ICP control (Rossaint et al. 2009)
-
Choice of agent individualized, used in context of institutional expertise
-
-
Barbiturates
-
Theory: reduce cerebral metabolic demands.
-
Delayed effects
-
Not in ED
-
-
Steroids
-
Popular in past
-
High dose methylprednisolone assoc. w/ increased mortality (Brain Trauma Foundation et al. 2007d), CRASH 2004 trial
-
-
Temperature Management
-
Maintain normothermia with antipyretics
-
Hypothermia
-
Topic of current study: Associated with mortality in trauma. Maybe neuroprotective.
-
Meta-analysis by Brain Trauma Foundation: hypothermia for 48 hrs reduction in mortality. *small sample size (Brain Trauma Foundation et al. 2007b)
-
Ongoing trial in Europe: “Eurotherm3235 Trial (Sinclair and Andrews 2010)
-
-
-
Glucose Management
-
Avoid hyper (<180 mg/dL) and hypoglycemia
-
-
Prophylactic Antibiotics
-
Indications: penetrating head injury, open skull fracture, complicated scalp laceration
-
“May be used but are not recommended” with only otorrhea or rhinorrhea (Marx et al. 2006)
-
-
Recombinant factor VIIa
-
Hemostatic agent for hemophilia
-
Area of investigation
-
Not sufficient evidence to recommend
-
-
Hyperventilation
-
Goal normocarbia PCO2 to 30-35 mm Hg
-
Onset in 20 seconds
-
Peaks in 8 min
-
Lowers ICP 25%
-
Prolonged hyperventilation causes vasoconstriction and ischemia
-
Short term lifesaving if herniation
-
However guidelines recommend avoiding in acute phase
-
-
Cranial Decompression
-
Rapidly deteriorating in ED: consider burr hole as bridge to OR craniotomy
-
“Talk and deteriorate”
-
Blind procedure
-
Better change if localizing lesion
-
Unconscious, symmetric pupils – unlikely focal lesion amenable to emergency decompression
-
Renewed interest among the neurosurgical literature for emergent decompressive craniectomy…
-
-
Seizure Prophylaxis
-
Seizures -> hypoxia, hypercarbia, increased ICP.
-
Post-traumatic seizures (PTSs) 12% with blunt trauma, 50% with penetrating head injury.
-
Active seizure -> treat:
-
Lorazepam 0.1mg/kg IV up to 4mg
-
Fosphenytoin 20 mg/kg (faster, less fluid, less hypotension than phenytoin)
-
-
Evidence for prophylaxis:
-
Cochrane Review 2015: NNT 10 to prevent early seizure. (Thompson et al. 2015)
-
Other evidence suggests no long term changes in outcome. (Khan and Banerjee 2010)
-
-
Indications for prophylaxis:
-
Depressed skull fracture, paralyzed and intubated, seizure at injury or in ED, penetrating brain injury, GCS <=8, subdural, epidural, intracranial hemorrhage, hx of seizures
-
Paralytics may obscure ability to realize seizureform activity
-
Prophylactic levetiracetam (Keppra) 20 mg/kg load, 1g BID or phenytoin (Dilantin) 20 PE/kg load, 100 PE TID x 7 days (paucity of literature)
-
-
-
Priorities
-
Immediate surgical intervention for chest or abdominal injury, head injury evaluation may be curtailed.
-
Patients may be too unstable for head CT before surgical intervention.
-
Neurosurgical consultation for clinical evaluation for intraoperative ventriculostomy or bilateral trephination with post-op CT.
-
-
Neurosurgical Interventions
-
Guidelines for evacuation epidural, subdural, intracerebral hemorrhage.
-
“While ICP monitoring has long been central to the management of patients with severe head injury, the strength of this recommendation has been limited by lack of large randomized trials.” (“Management of Acute Severe Traumatic Brain Injury” 2017a)
-
Beyond scope of this talk
Specific Topics of Debate (Past and Present)
-
Coagulopathies
-
Coags upon presentation.
-
Warfarin -> P4-factor PCC (Kcentra) or FFP (15 mg/kg) and vitamin K.
-
Thrombocytopenia -> transfuse to > 75k.
-
If on antiplatelets (ASA, clopidogrel):
-
Effect of platelet transfusion is not known. (Nishijima et al. 2012)
-
Expert opinion (Harbor NS, Weingart, 2013):
-
Single-donor packed platelets (6-pack)
-
ddAVP 0.3 mcg/kg
-
-
Clinical review of literature (Campbell et al. 2010) algorithm:
-
ASA alone, give 5 units
-
Dual anti-platelet therapy and large ICH 1-2 donor packs of platelets and ddAVP*
-
ddAVP promotes vWF production but side effects include hyponatremia, seizures, and elevated ICP (Campbell, 2010) and (Kim, EMDocs, 2014)
-
-
-
-
Osmotic Agents
-
Brain Trauma Foundation and European Brain Injury Consortium recommend mannitol
-
Mannitol may be detrimental compared with HTS (Oddo et al. 2009)
-
Cochrane review of mannitol (Wakai, Roberts, and Schierhout 2007): 4 studies
-
ICP directed care to “standard care” RR for death 0.83%
-
Mannitol to pentobarbital. RR for death 0.85%
-
Mannitol to HTS. RR for death 1.25%
-
Prehospital mannitol to placebo. RR for death 1.75
-
-
Mannitol
-
0.25-1 g/kg q3 hours
-
Effect in minutes, peaks @ 60 min, duration 6-8 hrs
-
Other neuroprotective properties: Volume expander in hypovolemic hypotension, reducing blood viscosity, reduces microcirculatory residence, free radical scavenger.
-
Adverse effects: hypotension in high doses, renal failure, paradoxical increased bleeding into lesion by decompressing tamponade of a hematoma. Need to monitor osmolality, electrolytes.
-
Reserved for evidence of increasing ICP/neurological deterioration (Brain Trauma Foundation et al. 2007a)
-
-
Hypertonic Saline (HTS)
-
3 ml/kg (of 3%) over 10 min
-
7.5% with dextran 250 ml (Holmes, J. EB Medicine, 2013)
-
Used for TBI since 1919
-
Numerous studies with small n’s show reduction in ICP.
-
Adverse effects: renal failure, central pontine myelinolysis, rebound ICP elevation
-
Large, multicenter, double-blinded, randomized, placebo-controlled study: no improvement in neurologic outcome with prehospital HTS (Bulger et al. 2010)
-
-
Impression: Not indicated empirically. Indicated when herniating.
-
Which one:
-
-
Lidocaine (thought to have prevented hypertensive responsive, cough reflex, increased ICP). No benefit from use of non-depolarizing neuromuscular blocking agent to prevent transient elevation in ICP with fasciculations (Clancy et al. 2001). Impression: Ensure adequate sedation instead.

-
Subparalytic dose of nondepolarizing agent to prevent succinylcholine’s fasciculations from causing increased ICP
-
Succinylcholine v. rocuronium for RSI in TBI.
-
TBI is NOT absolute contraindication to succinylcholine
-
Succinylcholine is associated with increased mortality when used for rapid sequence intubation of severe brain injured patients in the emergency department. Patanwala. Pharmacotherapy 2016; 36(1) 57-63. PMID: 26799349
-
Retrospective. Insufficient evidence.
-
No mention of it even in UpToDate
-
-
-
Etomidate v. Ketamine
-
Etomidate reduces CBF and metabolism [Anaesthesia study ‘92] (Marmarou et al. 2007; Bar-Joseph et al. 2009; Bernard et al. 2010; Fakhry et al. 2006; Modica and Tempelhoff 1992)
-
Etomidate best hemodynamic profile [review 02] (Yeung and Zed 2002)
-
EMDocs: “Ketamine has not been shown to increase ICP in recent studies. The original studies concluding an increase in ICP were done on small numbers of patients, and the patients were given far greater doses of ketamine than are provided during your standard RSI. Therefore, they did not bear out in clinical practice. In fact, due to ketamine’s blockade of reuptake of catecholamines, it maintains both MAP and CPP, preventing hypoxic and hypotensive episodes, which are more common and devastating dangers to head injury patients.” (http://www.emdocs.net/ketamine-and-rocuronium-the-new-etomidate-and-succinylcholine/)
-
Ketamine does cause release of catecholamines. If hypertensive or normotensive and TBI, “should probably” be avoided. If hypotensive, ketamine or etomidate recommended.(Marx et al. 2006)
-
-
Reminder: IM exists
-
succinylcholine 4 mg/kg IM with 2-4 min onset (4-5 min children)
-
ketamine 4 mg/kg IM OR midazolam 0.1-0.3 mg/kg IM
-
-
Decompressive LP
-
TBI Prognostic Factors
Resources:
-
Brain Trauma Foundation: https://www.braintrauma.org/
-
Reference Notes
-
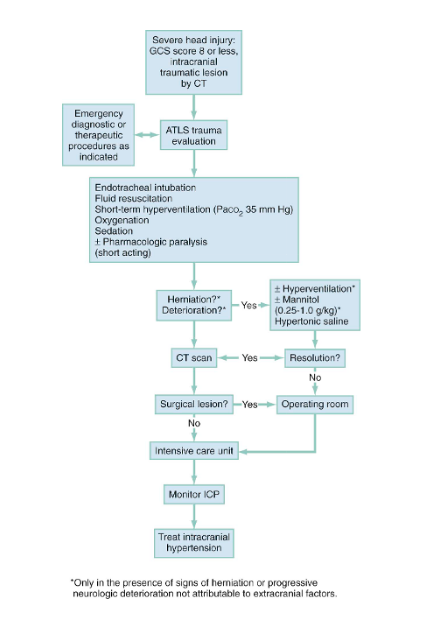
Decision Tree from Rosen’s:
-
Reading Head CTs:
-
http://medtx.org/wp-content/uploads/2017/05/5d5d3732b4a1bd24f0a88a37fc9cbefb.pdf
-
-
CT reading room: place to close loop for findings, plan, who calls consults, and MD-RN communication.

References
-
“Management of Acute Severe Traumatic Brain Injury.” 2017a. Accessed May 9. https://www.uptodate.com/contents/management-of-acute-severe-traumatic-brain-injury?source=search_result&search=traumatic%20brain%20injury&selectedTitle=2~150.
-
———. 2017b. Accessed May 9. https://www.uptodate.com/contents/management-of-acute-severe-traumatic-brain-injury?source=search_result&search=traumatic%20brain%20injury&selectedTitle=2~150.