Intubation:
RSI
-
- Etomidate 20mg (0.3mg/kg)
- Sux 100mg (1.5mg/kg) – starts 45 sec, lasts 6-10 min.
- Rocuronium 80mg (1.2mg/kg). 75 sec onset. lasts 33 min. sugammadex, 16 mg/kg IV reversal.
- ketamin IM 5mg/kg for immediate sedation (be prepared to manage airway)
- propofol inducation 1.5-2 mg/kg (avoid w/ soy and egg allergy)
- 1/2 dose sedatives in hemodynamically unstable patient.
- If IM:
- succinylcholine 4 mg/kg IM with 2-4 min onset (4-5 min children)
- ketamine 4 mg/kg IM OR midazolam 0.1-0.3 mg/kg IM
- Push dose pressors
- Rules of 10s: take 10cc flush, squirt out 1 cc, fill with 1 cc of 1/10k epi. = 10mcg/cc of epi. So pushing 1 cc’s every 1 min would be about 10mcg/min. Dose of gtt is 0.1 to 1 mcg/min/kg. So for 100kg person, 1 cc per min is the lowest (0.1mcg/min/kg) and pushing all 10 cc per min would be max (1mcg/min/kg). So basically pushing anywhere from 1 to 10 cc/min is equivalent to the normal range.
- Epi: 1/1000 is IM form. 1/10,000 is IV form (for ACS)
- Quick epi gtt: Take your code-cart epi (it doesn’t matter if it’s 1:1,000 or 1:10,000) and inject 1mg into a liter bag of NS. Final concentration is 1mcg/ml. Run at 1cc/min and titrate to effect” Run side open which will be with an 18 gauge IV about 20cc/min which is 20mcg/min. 20 drops is 1 cc. quoted from WikEM. Also article on ALiEM.
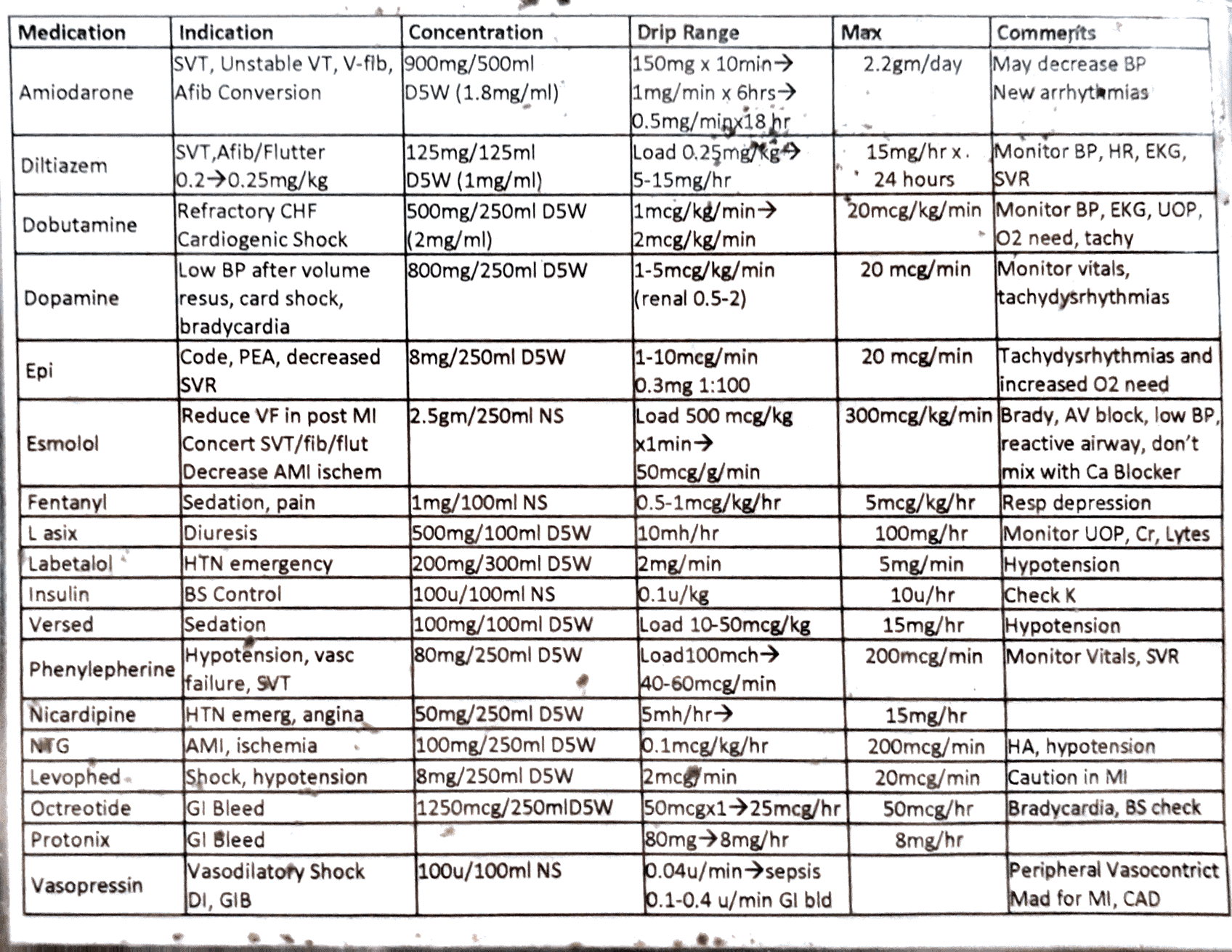
- Drips
- Norepinephrine 10mcg/min (max 30) then second line pressor.
- Dobutamine first line if CHF. Start 2.5 mcg/kg/min. Range 10-40.
- Propofol for maintenance intubation: 5 mcg/kg/min.
- 0.001mg=1mg (3 decimal places)
-
Imaging (Clinical Decision Rules, Courtesy of WikEM)
- Canadian C-Spine (GCS 15, Hemodynamically stable, Age <16)
- High Risk Rhyme
- Sixty five,
- Fast drive (dangerous mechanism), Sense deprive (Image if alive), Low Risk Rhyme, Slow wreck, Slow neck, Sitting down, Walking around, C-spine fine
(Range the spine) - No High Risk Factors
- Age >65
- Dangerous mechanism
- Parasthesias in extremities
- ANY Low Risk Factor
- Simple rear end MVC
- Delayed onset of pain
- Sitting position in ED
- Ambulatory at any time
- Absence of midline C-spine tenderness
- ROM
- Rotates neck 45 degrees to left and right
- C-spine can be cleared clinically if above criteria met[3] [4]
- Canadian Head CT
- Inclusion Criteria
- GCS 13-15
- Age ≥ 16yr
- No coagulopathy nor on anti-coagulation
- No obvious open skull fx
- Rule
- Head CT not required if NONE of the following are present
- Age ≥ 65 years
- Vomiting > 2 time
- Suspected open or depressed Skull Fracture
- Signs suggesting basal skull fracture:
- Hemotympanum
- Racoon eyes
- CSF otorrhea or rhinorrhea
- Battle’s sign (bruising around mastoid process)
- GCS < 15 at 2 hours post injury
- Retrograde Amnesia > 30min
- Dangerous mechanism
- Pedestrian struck by vehicle
- Ejection from motor vehicle
- Fall from elevation >3 feet or 5 stairs
- Canadian C-Spine (GCS 15, Hemodynamically stable, Age <16)
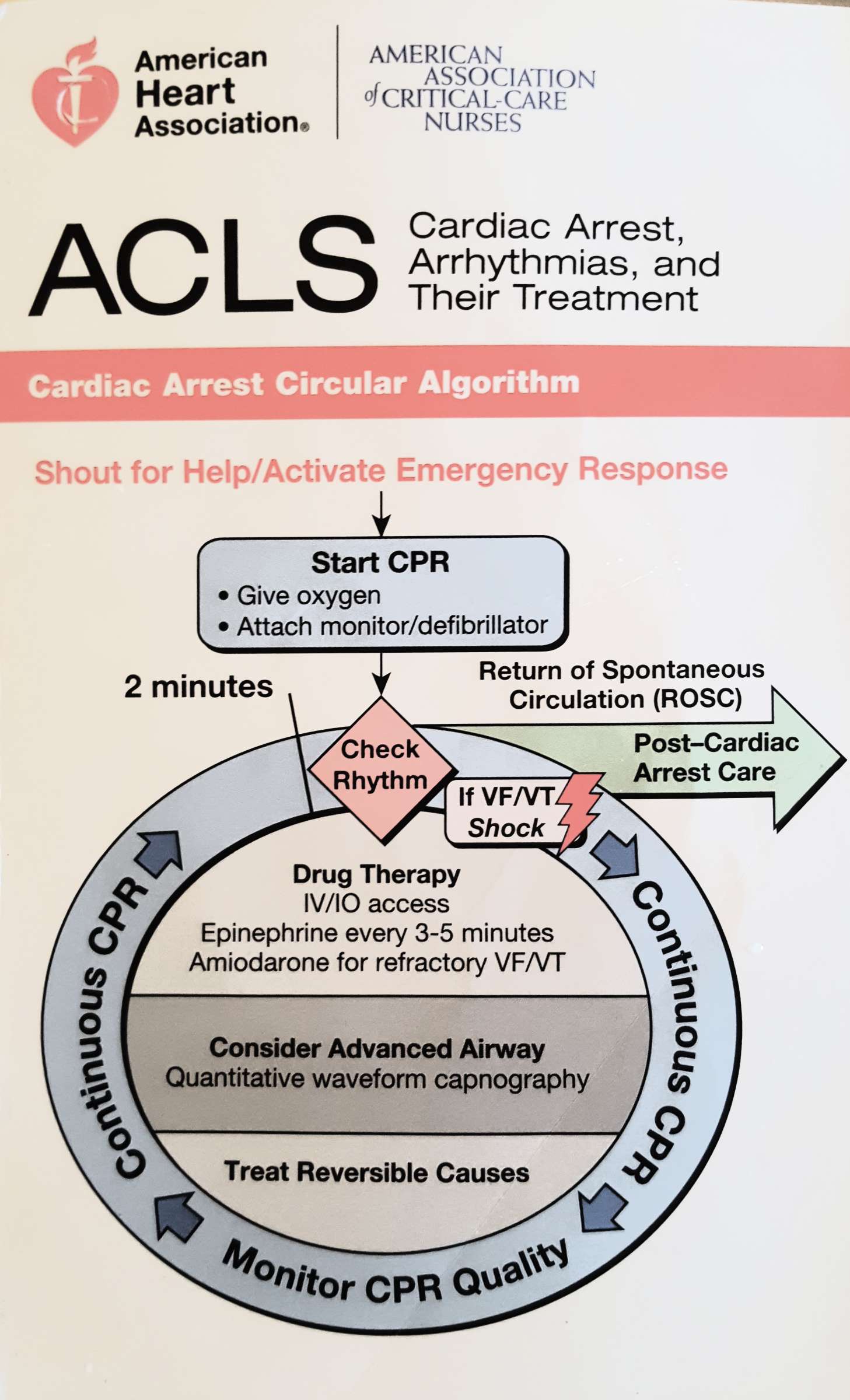
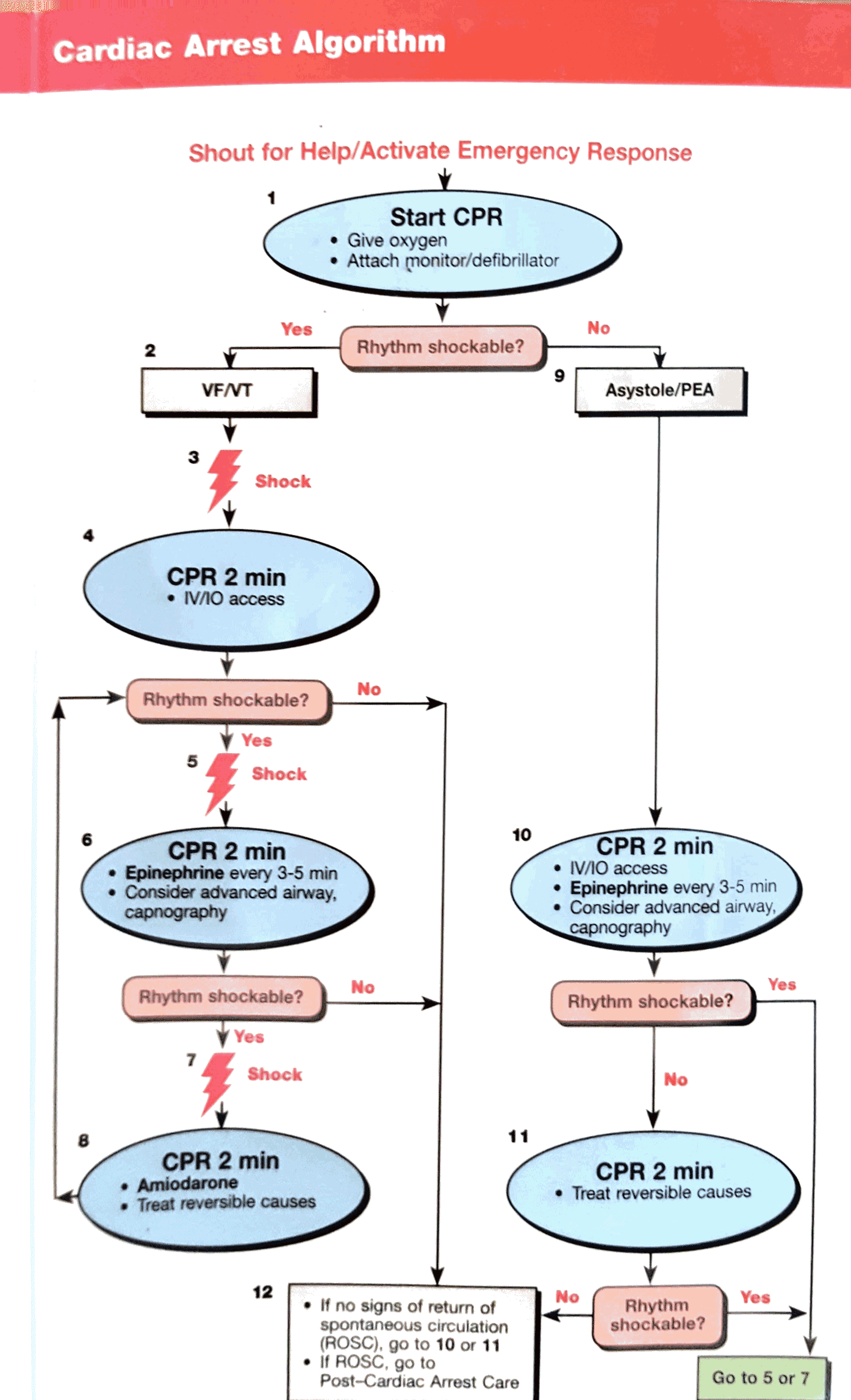
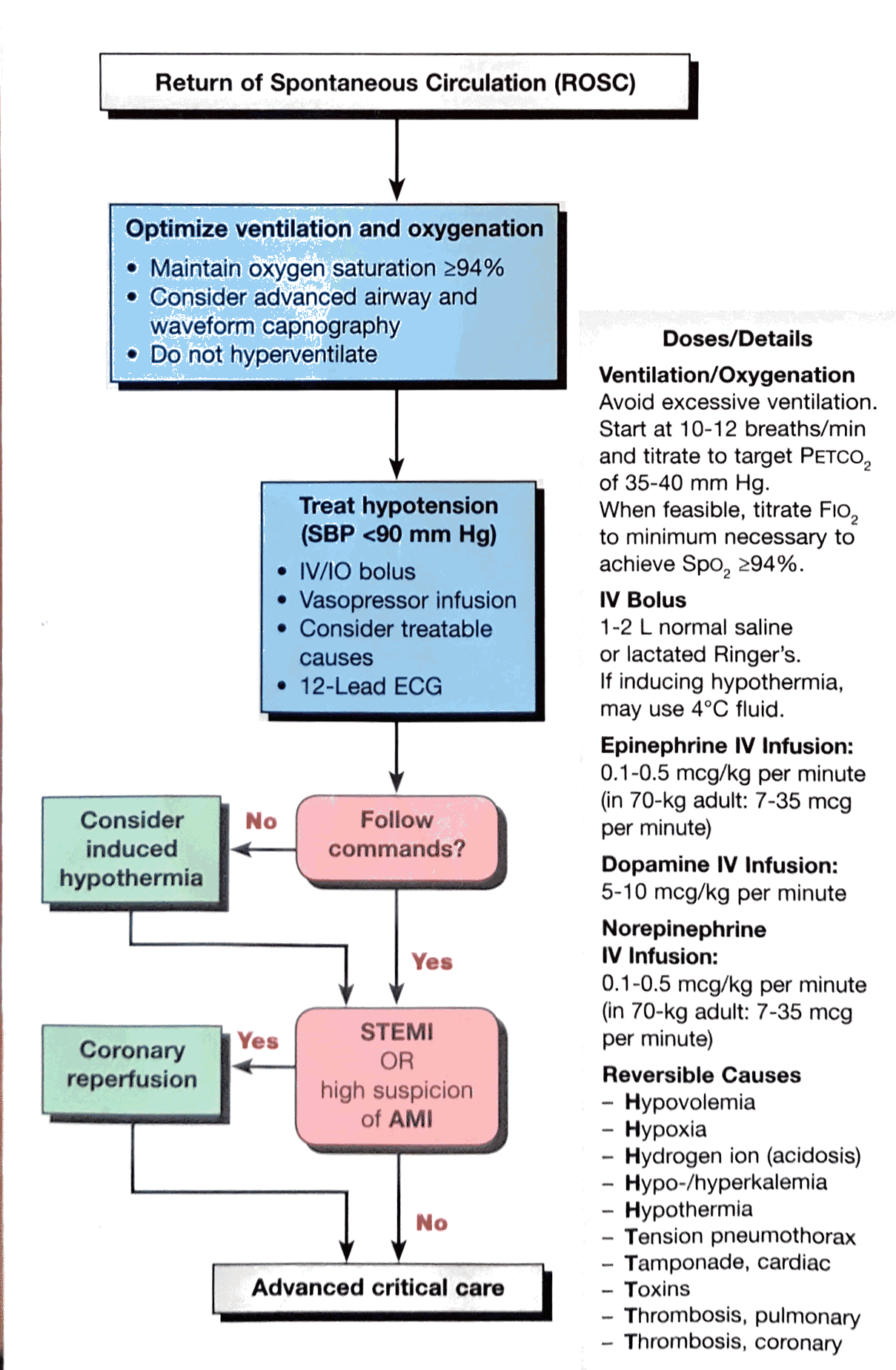
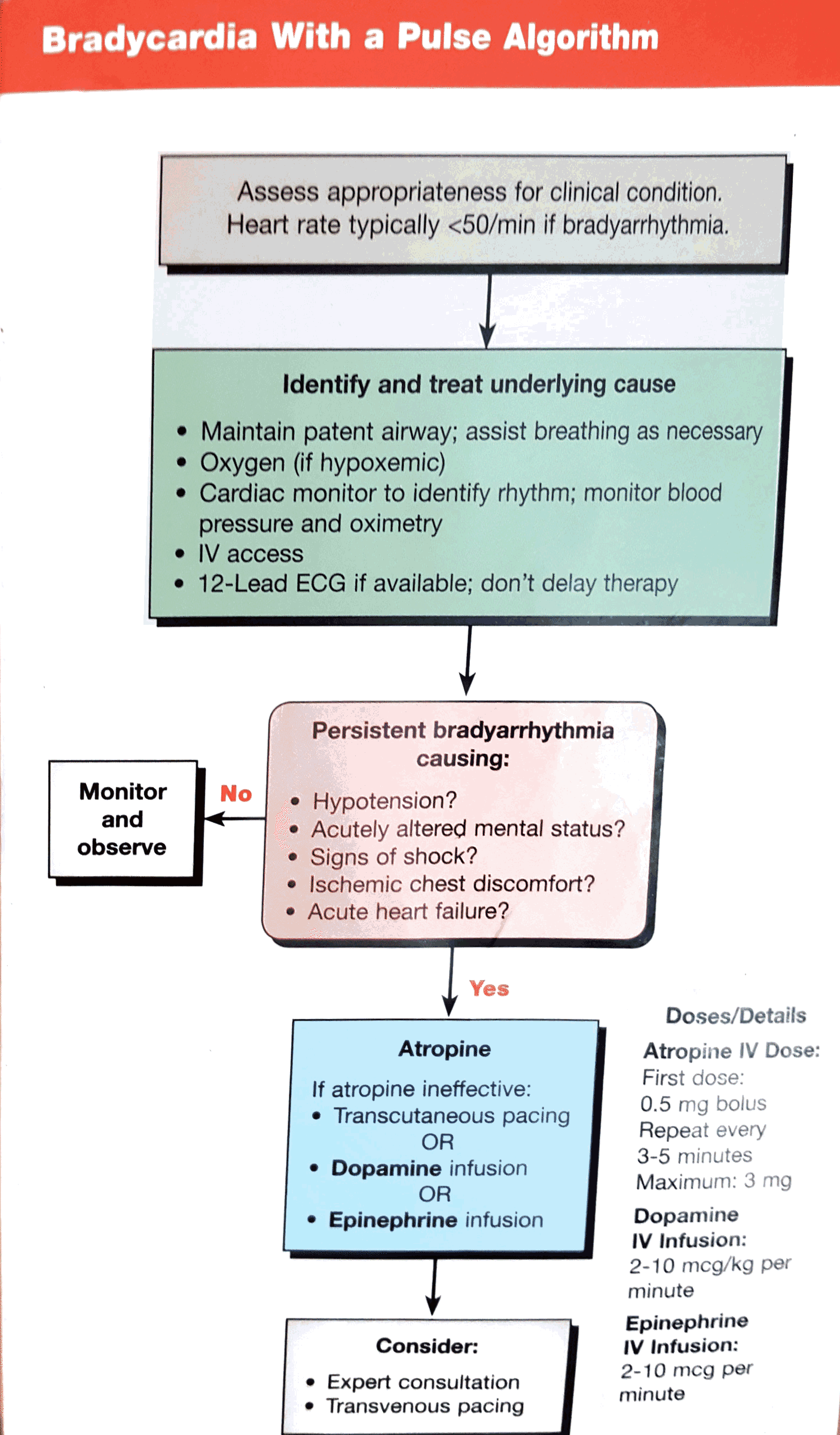
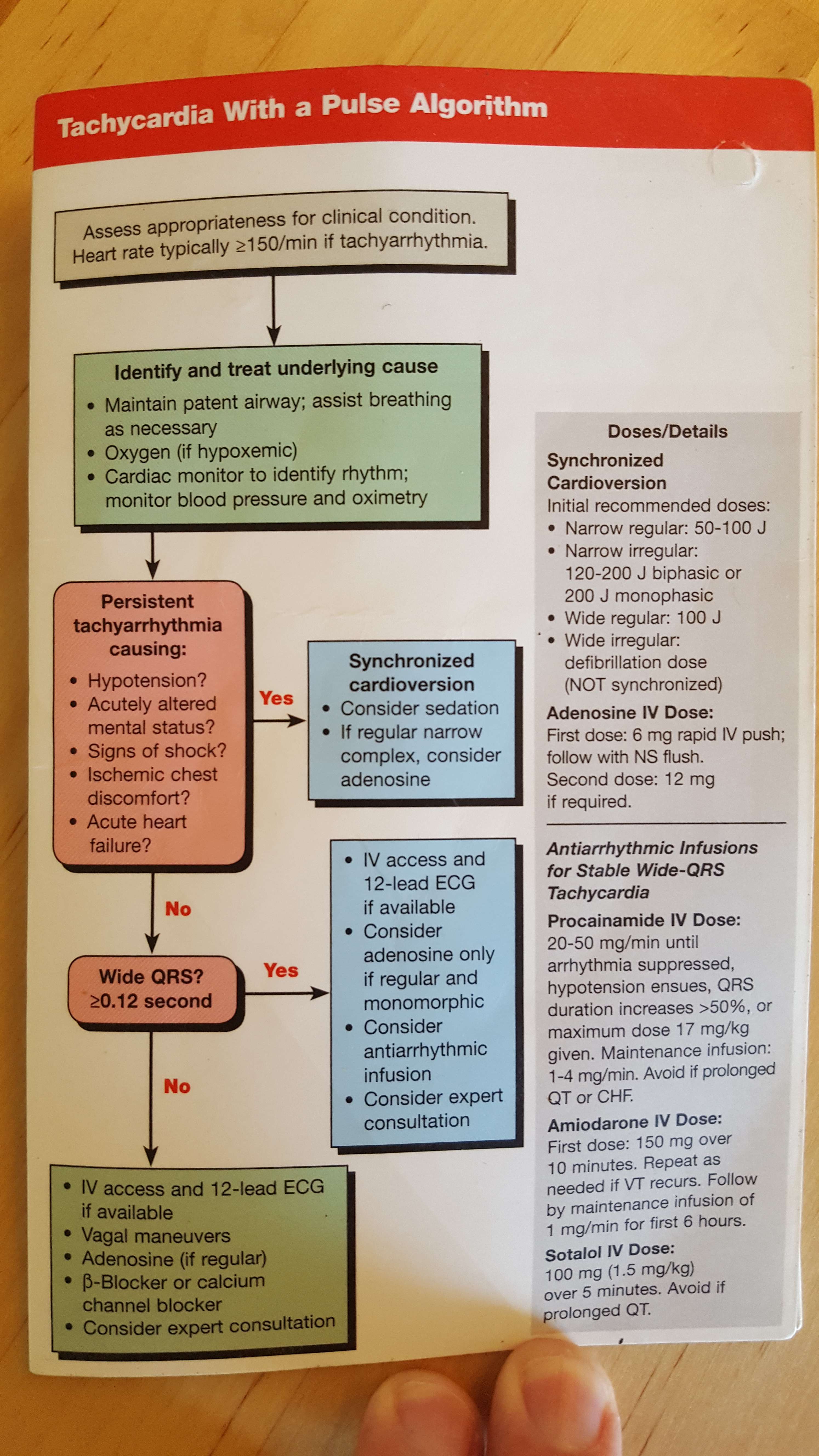
- AHA
*This information is intended for educational purposes only and not intended for use in patient care (which requires a trained credentialed attending physician and individualization of the medical care plan to the specific patient).